Query
What are the latest best practices for addressing and mitigating corruption in public health procurement? Please provide evidence from around the world and, if possible, from the Central Asian region.
Background
Public health procurement refers to the process through which governments purchase medicines, medical supplies, equipment and services, as well as commission the construction and maintenance of health infrastructure to deliver healthcare (Transparency International n.d.). When managed through transparent, competitive and accountable processes, public health procurement can advance universal health coverage (UHC) and the Sustainable Development Goal on health (SDG 3), by contributing to an efficient use of public resources and promoting equitable and timely access to medicines, technology and services.4a1a7e19687b
These global commitments are complemented by international governance frameworks and technical standards that guide how health procurement systems should operate in practice. For example, the World Health Organization (WHO) provides a normative framework that procurement processes should align with, including the operational principles for transparent and efficient pharmaceutical procurement7e83027b335e (WHO 1999). The WHO also sets technical standards, including for manufacturing practices (WHO 2022a), distribution (WHO 2010), and storage, with which procurement and supply chain processes must comply when selecting suppliers and verifying product quality.
In many low- and middle-income countries, including in Central Asia5fdb93ebe588, procurement financed by international development partners is further governed by specific integrity and transparency requirements.These include the World Bank's Procurement Regulations for Investment Project Financing, which establishes core principles of value for money, integrity and competitive procedures applicable to all projects financed by the Bank (World Bank 2025). The Global Fund and Gavi also impose strict procurement and quality assurance requirements on grant recipients, including mandatory product prequalification and supplier eligibility criteria (The Global Fund 2019; Gavi 2023). These frameworks constitute an additional layer of accountability in countries where donor-financed procurement represents a significant share of total health expenditure, in a sector whose overall scale makes it a particularly high-stakes area for governance.
Public procurement represents between 12% to 20% of gross domestic product (GDP) globally (OECD 2025b: 147). Across OECD countries, health is the largest sector for public procurement, comprising nearly one third of total government procurement spending, estimated at approximately 32% in 2021 (OECD 2025b: 146). Comparable sectoral breakdowns are not available for non-OECD countries, however, WHO data on government health expenditure confirms that health constitutes a substantial share of public spending across 195 countries (WHO, 2025). On this basis, health procurement is widely understood to represent the largest single category of public procurement globally, making it a significant sector in public financing and, consequently, particularly vulnerable to corruption and mismanagement.
Central Asian countries91ed29e94ed3 face persistent challenges in public health procurement. Government health expenditure remains low across the region, ranging from approximately 0.94% of GDP in Turkmenistan to 2.48% in Kazakhstan (WHO GHED, 2023), well below OECD averages and the WHO-recommended threshold for sustainable health financing (Shaltynov et al. 2021). Out-of-pocket (OOP) spending in the region is higher than the OECD average of 20%, ranging from over 77% of total health expenditure in Turkmenistan to around 28% in Kazakhstan (WHO GHED, 2023). High OOP spending can be both a symptom and a driver of corruption: corrupt procurement practices waste scarce resources on overpriced or unnecessary goods, while bribes and informal payments force patients to pay out of their own pockets for services that should be free or low-cost (Albisu Ardigó and Chêne 2017). These structural weaknesses create fertile ground for broader procurement corruption: OECD monitoring consistently identifies public procurement as among the sectors most affected by embezzlement and abuse of office in the region (OECD 2020).
Understanding corruption in public health procurement
According to Transparency International’s definition, corruption in procurement refers to the abuse of entrusted power for private gain in the acquisition of goods, services or works (Kühn and Sherman 2014: 6). The combination of high financial value, complex technical specifications, and multiple public and private actors makes health procurement particularly vulnerable to corruption (Kohler and Dimancesco 2020:2; Onwujekwe et al. 2020: 5-6). Article 9 of the United Nations Convention against Corruption (UNCAC 2004) specifically requires state parties to establish transparent and competitive procurement systems based on objective criteria, effective review mechanisms, and accountability safeguards.f4f2f7f33ecd
In public health, corruption may occur at any stage of the procurement cycle and can compromise competition, transparency and fairness. In pharmaceutical markets in particular, limited competition and patent protections strengthen suppliers’ bargaining power (Pogge 2023: 199; Wemos and Health Action International 2025), while limited price transparency makes it more difficult to detect inflated costs or other forms of market manipulation. Pharmaceutical markets are also susceptible of collusive arrangements among suppliers, including cartel behaviour in which competing firms coordinate bids or prices to manipulate procurement outcomes and further suppress competition (OECD 2020a; García Rodríguez 2022). Confidentiality and non-disclosure clauses in drug procurement contracts further shield key pricing and supply terms from public scrutiny, limiting benchmarking among purchasers and weakening accountability. For example, in South Africa, a court-ordered disclosure of COVID-19 vaccine contracts revealed that pharmaceutical companies had charged the government higher prices than those paid by the European Union for the same vaccines. These price disparities had been concealed from public scrutiny through confidentiality clauses (Cullinan 2024; Veljanov and Fazekas 2023).
While decentralised systems, where procurement responsibilities are dispersed across hospitals and regional authorities, may increase discretion and reduce effective oversight (OECD 2016:7), centralised systems can generate different but equally significant risks. Where decision-making power is concentrated and accountability mechanism such as checks and balances are weak, limited transparency and close relationships between public officials and private suppliers may create structural opportunities for state-capture and corruption in procurement decisions (Rose-Ackerman and Palifka 2016). Collusion may also be sustained through vertical corruption, where firms rely on insiders within procurement agencies to protect cartel arrangements or manipulate tender outcomes (Auriol et al. 2016). These risks are particularly salient in transitional governance contexts where oversight institutions may lack independence or enforcement capacity.
In Central Asia, public procurement systems are largely centralised, often structured around unified e-procurement platforms (Kazakhstan and Uzbekistan) and dedicated state procurement agencies (Kyrgyzstan and Tajikistan). Tajikistan is consolidating procurement through a single e-procurement portal, while in Turkmenistan procurement reforms and digitalisation appear less advanced (World Bank Global Public Procurement Database). Public procurement systems have undergone significant legal reform over the past decade. Countries such as Tajikistan and Uzbekistan have aligned their procurement laws with international standards, including to Article 9 of UNCAC and OECD Recommendation on Public Procurement (2015), which call for transparent and competitive procurement systems and safeguards throughout the procurement cycle. Tajikistan, for example, has invested in strengthening regulatory frameworks and expanding automation and transparency measures (Djumaev 2023). However, OECD assessments under the Istanbul Anti-Corruption Action Plan (IAP)cc4476f9c98a (OECD 2024a) indicate that implementation and enforcement remain uneven across the countries reviewed in the region, highlighting some gaps.
Table 1: Examples of key public procurement gaps highlighted in the Fifth Round of Monitoring of Anti-Corruption Reforms under the Istanbul Anti-Corruption Action Plan
|
Kazakhstan |
Kyrgyzstan |
Tajikistan |
Uzbekistan |
|
|
|
|
Sources: OECD 2024a, OECD 2024b, OECD 2024c and OECD 2024e.
Although Turkmenistan is not part of the IAP, similar challenges have been acknowledged. There is reportedly an excessive reliance on single-source contracts, limited competition, and weak enforcement of transparency and oversight measures (Business Turkmenistan 2024).
Impact of corruption in public health procurement
Corruption in health procurement has significant fiscal and public health consequences. The WHO estimates that corruption, fraud0e2fd63678c7 and waste in health account for approximately 7.3% of global health spending00baf30f9ee5 (WHO 2023). This is a combined estimate covering multiple forms of inefficiency; based on pre-COVID-19 financing levels, it amounts to roughly US$455 billion, far exceeding the estimated US$370 billion per year required to achieve universal health coverage (WHO 2023). Considering that procurement constitutes a substantial share of health expenditure and is among the areas most vulnerable to corruption, the scale of the problem becomes evident. Such losses are associated with reduced availability of essential medicines, inflated prices, stock-outs, the circulation of substandard or falsified products, and the distortion of health priorities away from population needs (Seidman and Atun 2017; Onwujekwe et al. 2020). Statistical analyses also link higher levels of perceived corruption with poorer health outcomes, including higher child mortality (National Academies 2018).
Beyond financial losses, corruption erodes public trust and undermines compliance with public health policies. For example, in Kyrgyzstan, the health minister’s procurement of unneeded COVID-19 vaccines and the embezzlement of funds into offshore accounts exemplified the government mismanagement of the pandemic. This fuelled popular protests and deepened public mistrust in government, resulting in lower adherence to COVID-19 mitigation measures and widespread vaccine scepticism (Grant 2024: 266).
By diverting limited public funds away from essential medicines and services, inflating costs, and creating shortages of quality supplies, corruption in public health procurement disproportionately affects those facing systemic barriers. People living in poverty, women, children, rural communities and other marginalised groups face greater obstacles to accessing care, worse health outcomes, and higher out‑of‑pocket costs compared with better‑off groups (Steingrüber Harris 2017). In Uzbekistan, journalists uncovered that the Ministry of Health paid nearly twice the retail price for a medicine through a deal allegedly linked to a former minister. Corrupt procurement in this case resulted in the mass poisoning of over 70 children in 2023 (OECD 2024d: 198).
Ultimately, corruption in health procurement undermines availability, quality and equity in healthcare, exacerbating inequities (Onwujekwe et al. 2020; Wong et al. 2024). It is, in this sense, a governance and a public health challenge, but it can also undermine states’ obligations to realise the right to health recognised in Article 12 of the International Covenant on Economic, Social and Cultural Rights (United Nations 1966; CESCR 2000: paras. 1–3, 43–45).
This Helpdesk Answer synthesises available evidence on approaches to address and mitigate corruption risks in public health procurement, with reference where possible to examples from Central Asia. Nonetheless, the evidence base remains uneven. Research has focused predominantly on pharmaceutical procurement, particularly medicines and vaccines, with comparatively limited attention to medical devices, despite recognised risks in these areas (Rose-Ackerman and Tan 2014; Ardigó and Chêne 2017). Many studies rely on proxy indicators, such as pricing trends or levels of competition, rather than direct measurements of corruption (Nemec et al. 2023). Where possible, this analysis distinguishes between evidence of implementation and evidence of demonstrated effectiveness.
Lastly, there is a lack of systematic studies and comparable data on corruption in health procurement across Central Asian countries. This report utilises government and media reporting to give examples of corruption in this sector. However, this also offers an incomplete picture, especially given low levels of media freedom in the region.139915e59c4c For example, the fact there are more reports of corruption scandals in health procurement in Kazakhstan than Turkmenistan may reflect the greater media openness in the former rather than the scale of corruption.
Corruption risks across the procurement cycle
Corruption risks arise at every stage of the procurement cycle, including in the health sector. While public health procurement presents specific vulnerabilities, as discussed in the previous section, these risks can still be systematically analysed using the standard procurement cycle framework. Corruption risks are commonly mapped across three stages: pre-bidding, bidding and contract award, and post-award contract management (Kohler and Dimancesco 2020: 3).
However, in health procurement contexts, this standard framework may require adaptation to capture risks that arise before the formal cycle begins, particularly where procurement operates through single state-owned distributors or is subject to tightly controlled supplier eligibility requirements. As illustrated in Figure 1, the three procurement stages are complemented by a preliminary stage covering stakeholder requirements, including supplier eligibility and conflict of interest declaration and management. This is particularly relevant in the Central Asian countries reviewed here, where such structural conditions are prevalent.
Figure 1: The procurement process
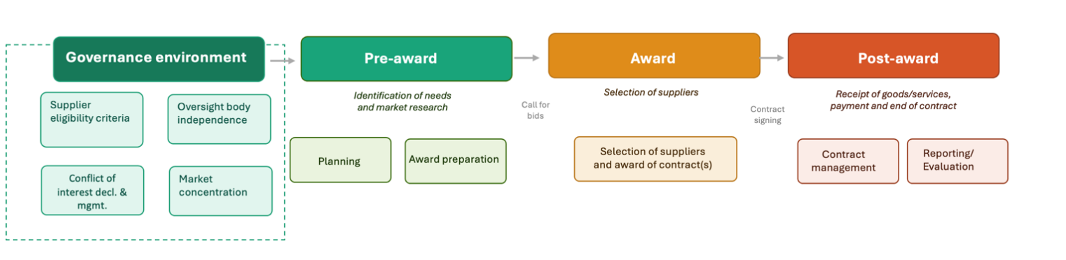
Source: Adapted from Patrucco and Dimand (2023)
Pre-bidding stage
The pre-bidding stageinvolves assessing needs, defining technical specifications and selecting procurement modalities. Decisions made at this stage, such as what to buy, how to define requirements and which procurement method to use, can shape who is able to compete and determine the winner before bidding even begins (Kohler and Dimancesco 2020; OECD 2016).
Documented corruption risks include manipulated needs assessment, biased specifications that favour specific suppliers, information asymmetries that grant privileged access to selected bidders, politicised priority setting, and the unjustified use of emergency or simplified procedures (OECD 2016; UNODC 2013; Morgner and Chêne 2014: 2). In pharmaceutical procurement, information asymmetries between suppliers and public authorities heighten these risks (Paschke et al. 2018; Onwujekwe et al. 2020). These practices distort competition among bidders and weaken transparency, thereby creating favourable conditions for bribery, collusion, patronage, and other forms of procurement corruption.
In Central Asia, policies provide procurement advantages to domestically produced medicines and equipment, which may increase the risk of additional eligibility criteria that, like specifications, can be manipulated to restrict competition before the tender opens (OECD 2016; OECD 2025a).
For example, in Kazakhstan, where domestic manufacturers are typically prioritised over foreign suppliers in state pharmaceutical tenders,investigations found that suppliers falsely claimed domestic production status for imported medical devices to gain eligibility and secure public contracts. Kazakhstan's Supreme Audit Chamber found that at least eight companies had made false domestic origin claims for medical supplies, and a criminal investigation was opened against one supplier of glucometers and test strips to the state distributor SK-Pharmacy (Orda.kz 2025; Times of Central Asia 2025).
Bidding and contract award stage
The bidding and contract award stage includes the publication of tender invitations by the relevant public institution or agency, the evaluation of the bids received, and the formal award of the contract(s). Recurrent corruption risks at this stage include bribery to influence bidding, undue influence of evaluation committees, and discriminatory disqualification of otherwise compliant bids. Risks that lead to corruption include non-competitive procedures, which create opportunities for favouritism, bid rigging or kickbacks; conflict of interest, which may increase the likelihood of corrupt acts such as favouritism; vague or subjective standards for evaluating bids, which also facilitates favouritism; political interference, which can include bribery or fraud; and overuse of direct or simplified procedures, which increases the risk of corrupt practices, although overuse alone is not necessarily corruption. (UNODC 2013; Bruckner 2019). These risks may manifest through breaches of confidentiality or procedural manipulation that advantage certain bidders over others (Morgner and Chêne 2014: 2).
A documented example of such dynamics occurred in Uzbekistan, where a UK-based shell-company produced false documents to secure a lucrative government contract for essential healthcare equipment.This example highlights systemic weaknesses not just in Uzbekistan, but also in the UK, where money laundering and opaque corporate structures allow politically connected individuals to exploit loopholes and channel illicit funds with minimal risk of detection in countries with weaker oversight (Leask 2021). More recently,in Kyrgyzstan, a procurement irregularity was identified at the state-owned enterprise Kyrgyzpharma, where medicines were purchased at nearly double the price offered by foreign suppliers in competitive bids. Investigations revealed that higher-priced contracts were awarded to politically connected suppliers, indicating deliberate manipulation of procurement procedures to favour certain vendors (Argumenti 2026).
Quantitative procurement research, analysing large scale procurement datasets using statistical methods, also highlights structural red flags that may signal reduced competition or collusive arrangements (Fazekas and Tóth 2016). These include persistently low numbers of bidders or repeated awards to the same firms. While such indicators or red flags do not in themselves establish wrongdoing, they are widely used in risk-based monitoring. Another study in this field analysed public procurement data for pharmaceutical products in several countries, including Kazakhstan, and found corruption significantly inflated aggregate prices; it concluded that effectively addressing corruption risks could lead to a 19% price reduction in the products purchased in Kazakhstan (Veljanov and Fazekas 2023).
Post-award and contract management stage
Once the contract is awarded, there are still corruption risks. The post-bidding stage, covering the contract management, delivery, certification and payment, remains vulnerable to manipulation. For example, prices may be increased without justification, with additional work-orders can change significantly, or payment may be delayed unless bribes are paid. Substandard or falsified products may be certified as meeting standards. Weak enforcement of rules, lack of oversight, and ineffective complaint or sanction mechanisms make it easier for these practices to happen. In some cases, delays, misreporting, or improper approvals are used deliberately to benefit certain companies or individuals at the expense of fairness and public resources. (OECD 2016; Kohler and Dimancesco 2020).
In Honduras, for example, a civil society investigation led by Transparency International's national chapter uncovered that a supplier owned by a then-member of the national Congress delivered vitamin vials containing only four of the eleven specified active ingredients, at a volume below the contracted quantity. The products were initially accepted through the certification processes before quality testing intervened (Amin, 2018: 3). The company owners were subsequently charged with fraud, crimes against public health and falsification of documents.
Monitoring reports in Central Asia, particularly the Istanbul Anti-Corruption Action Plan for peer-reviewed monitoring, have similarly linked supply disruptions and reduced value for money to shortcomings in contract management and enforcement mechanisms (OECD ACN 2023). In Kazakhstan, for example, the authorities uncovered that hospitals and medical organisations had misused public funds through inflated procurement contracts, payments for services not rendered, and the delivery of medicines and equipment that never arrived. Funds were sometimes diverted via affiliated accounts, illustrating how weak contract oversight directly enables corruption and reduces value for money in healthcare (Aq Zhaiyq 2026).
Cross-cutting and structural risk factors
Beyond stage-specific vulnerabilities, procurement systems are shaped by broader governance factors and market conditions (Rose-Ackerman and Palifka 2016; Nemec et al. 2023). Regulatory capacity, independence of oversight bodies, market concentration and political influence over public administration all affect corruption risk exposure (Rose-Ackerman and Palifka 2016; Nemec et al. 2023). In hospital settings, for example, doctors’ requests for specific equipment may be influenced by informal relations with manufacturers and suppliers (Rose-Ackerman and Tan 2014; Ardigó and Chêne 2017).
Strong oversight does not reduce corruption risk in a straightforward way. Where oversight mechanisms are punitive or poorly calibrated, procurement officials may become reluctant to take decisions for fear of personal sanction, even when acting in good faith. For example, in South Africa, research by Wishnia and Goudge (2020) found that centralisation and an “authoritarian management style” of the public health budget led to opaque decision-making and hindered reform implementation, as well as negatively impacting the overall functioning of the health system. Moreover, this administrative caution can also itself create conditions for facilitation payments, as vendors seek to unblock stalled approvals informally. As Søreide (2014: 1) notes, strict control "can easily be seen as a sign of low trust that may suppress motivation and accountability". This is a dynamic that effective oversight design must account for alongside the need for independence and capacity.
These dynamics are further reinforced where the market structure itself concentrates risk. In several Central Asian countries, the dominant role of single state-owned pharmaceutical distributors, such as Kyrgyzpharmain Kyrgyzstan, compounds these risks: where one entity controls tender design, supplier evaluation and distribution logistics, the functional separation underpinning competitive procurement is structurally weakened, creating conditions conducive to elite capture (OECD 2024b: 90–98; Subkhanov 2023). The lack of a database to track beneficial ownership of companies participating in the bidding process creates additional risks across all stages. Beneficial ownership refers to the real individuals ("beneficial owners") who ultimately own, control, or benefit from legal entities such as companies or trusts. In the region, the absence of mandatory disclosure requirements in procurement eligibility frameworks often allows related-party contracting and politically connected ownership to go undetected, as illustrated by the shell company awarded a healthcare equipment contract in Uzbekistan (Leask 2021; OECD 2024b: 113–122).
At the higher levels of government, political corruption may distort any level playing field for health sector procurement. Peyrouse (2021) explains that in Tajikistan two large pharmaceutical companies are owned by members of the presidential family. They have allegedly exploited their political connections to restrict competition and sell pharmaceutical products at inflated prices.
Overall, the literature suggests that while procedural red flags are useful for risk detection, they do not fully capture structural drivers like elite capture, power asymmetries, and institutional weaknesses. These structural factors shape how procedural risks manifest in practice and may limit the effectiveness of technical safeguards if broader governance challenges are not addressed (Nemec et al. 2023).
Emergency procurement
Public health emergencies may intensify existing vulnerabilities in countries’ health procurement systems. During emergencies, vast resources are disbursed under pressure, often through accelerated procedures and waived requirements, or oversight (Kohler and Wright 2020: 2).
Emergency procurement regimes are special legal frameworks and procedures that allow governments and health authorities to bypass or simplify the normal purchasing process when there is an urgent situation of extreme urgency (such as a public health crisis or other emergencies) that requires a fast response. Rather than running a full competitive tender, buyers may award contracts directly, skip standard approval steps and reduce documentation requirements, all in the interest of speed (Griffore et al. 2023).
While these flexibilities are necessary in a crisis, they also concentrate procurement risks by design; accelerated procedures, direct awards, and reduced documentation requirements create conditions in which corruption risks increase significantly. The COVID-19 pandemic provided the most extensively documented illustration of these dynamics. During the COVID-19 pandemic in the UK, a “VIP lane” allowed politically connected suppliers to bypass standard scrutiny and receive preferential access to PPE contracts, with many contracts awarded without competition and some resulting in unusable equipment (Transparency International UK 2024).
In Central Asia, the risks were equally visible. In Uzbekistan, non-competitive contracts awarded to politically connected companies and COVID-19 response funds were embezzled from the national pandemic fund (Gogidze 2024: 10–11). In Kyrgyzstan, Transparency International's national chapter conducted a price analysis of medical supply procurement during the pandemic that documented significant overpricing (Transparency International Global Health 2023).
Approaches to mitigating corruption risks in health procurement
The preceding section mapped corruption risks across procurement systems and stages. Evidence suggests that effective mitigation requires addressing vulnerabilities at multiple stages and in different contexts simultaneously. Legal frameworks shape incentives and behaviours throughout the cycle; digital systems affect planning, tendering and implementation; and oversight institutions may intervene at multiple points (Robert Agwot 2024; Adam 2024:7; OECD 2019a: section 3). Accordingly, this section is organised thematically rather than strictly by procurement stage or governance structure, highlighting where specific stages of procurement are most directly affected.
Effective and competitive procurement designs
Legal and regulatory foundations promoting open, and competitive procedures primarily affect pre-bidding and bidding stages determine the strength of post-award enforcement.
Centralised, decentralised and pooled procurement
Centralised procurement consolidates purchasing authority within a single entity (e.g. Ministry of Health), while pooled procurement aggregates demand across multiple buyers to negotiate jointly with suppliers. Both are structural features that shape the conditions for open and competitive procedures at the pre-bidding and bidding stages and determine the institutional capacity available for post-award enforcement. Both approaches can reduce some corruption risks while simultaneously introducing others, depending on whether some foundational conditions are in place. For example, a clear legal framework, well-defined policies and procedures, adequate capacity of procurement agents, and controls on elite capture, including conflict of interest policies, beneficial ownership registries, and independent audit systems (OECD 2021: 47-52).
Seidman and Atun’s (2017) review finds that centralised tendering in low and middle-income countries is often associated with cost savings, reduced stockouts, and improved product availability (2017: 9-10), which may lower corruption risks (Kohler and Dimancesco 2020). However, they warn that poorly overseen centralised tendering can favour unvetted suppliers and cause stockouts, as observed in Kenya (Seidman and Atun: 3). Beyond operational failure, a critical risk of centralisation is that the concentration of procurement power may facilitate elite capture or state capture by concentrating power in a public authority and enabling politically connected actors to monopolise contracts at scale (Fazekas and Kocsis 2020: 1–3). Effective mitigation requires countervailing measures such as conflict of interest policies and beneficial ownership transparency, open contracting standards, and robust audit functions (OECD 2021: 47–52); without these, centralisation may reduce the number of corrupt transactions while increasing their individual scale.
In contexts such as Kyrgyzstan and Uzbekistan, where these countervailingsafeguards remain underdeveloped, the problems are systemic rather than model-specific. In Kyrgyzstan, the establishment of a centralised procurement entity (Kyrgyzpharma) aimed to consolidate purchasing for public medical facilities and reduce intermediaries. However, the OECD analysis indicates that risks arise from weaknesses in specification design (e.g. restrictive tendering), limited competition gaps in contract enforcement, and inadequate transparency and information disclosure that constrain oversight. (OECD 2024b: 90-98). These weaknesses do not suggest that decentralised procurement would necessarily lead to better outcomes: decentralised systems require the same safeguards, applied consistently across every administrative unit, and the same stronger governance foundations are needed regardless of the procurement model.
A similar pattern is evident in Uzbekistan, where broader governance weaknesses mean that the safeguards needed to make centralisation effective (i.e. transparency, accountability, independent oversight) remain underdeveloped. The Open Contracting Partnership’s (OCP) scoping assessment identifies weak centralised oversight, a persistently high share of single-source direct purchases, incomplete transition to e-procurement, and unilaterally drafted contracts that limit supplier recourse (Subkhanov 2023: 1). This illustrates a common transitional scenario: centralisation is pursued as a reform measure, but without the transparency and accountability infrastructure needed to prevent it from becoming a vehicle for the very capture it was meant to reduce. The problem lies in the loopholes of the legislative framework, including a five-day announcement window for competitive selections and broad presidential decree exemptions that effectively legalise single-source awards, but also in implementation and oversight failures. Electronic procedures required by law routinely go unenforced, no single body holds end-to-end jurisdiction from violation detection to prosecution, and civil society efforts to independently monitor procurement outcomes, including in the health sector, have been actively obstructed (Subkhanov 2023).
Pooled procurement mechanisms, including international arrangements such as the Global Fund’s Pooled Procurement Mechanism, are associated with lower essential medicine prices (Ferrario et al. 2017; Wang and Zahur 2025). By aggregating demand and standardising procedures, pooled procurement can also reduce corruption risks associated with fragmented purchasing, such as collusion and bid manipulation (OECD 2010). Like centralisation, pooled procurement often shifts rather than eliminates corruption risks. The key variables are how discretion and competition are structured within the arrangement: while pooling can reduce local-level favouritism, it concentrates decision-making power, increasing the stakes of high-level corruption where governance is weak. At the supplier level, this concentration can favour connected or less efficient firms, systematically distorting contract allocation (Decarolis et al. 2021). These mechanisms may introduce certain governance risks, which include longer lead times and reduced operational flexibility, conditions that can obscure accountability, create pressure for off-channel purchasing, and allow mismanagement to go undetected before adequate oversight can be applied (Wang and Zahur 2025). As with centralisation, pooled procurement can mitigate corruption only when arrangements are accompanied by strong transparency, clear rules, and safeguards that preserve competition and limit discretionary abuse (OECD 2021: 47-52).
Decentralised models of procurement are often associated with fractured and poor oversight which can create space for corruption to flourish at local levels2235a082fb4b (Millington and Bhardwaj 2017). Conversely, these models – as well as mixed models where certain functions are decentralised and others not- may serve as effective alternatives if they are well managed in certain settings, especially those with devolved governance systems which benefit from differentiated financing and planning processes (Millington and Bhardwaj 2017). One literature review cited studies from Bangladesh and Brazil where decentralised health systems were associated with improved local accountability and monitoring mechanisms (WHO 2018:20).
Competition and transparency
Open and competitive processes (e.g. open tendering as opposed to direct awards, pre-announcement, disclosure of decisions) are consistently associated with better financial outcomes (Nemec et al 2023; Amin 2017) and lower perceived corruption (Mahuwi and Israel 2024; Bayked et al. 2024). Large-scale analyses of procurement contracts across Central and Eastern Europe show that open procedures correlate with lower prices and increased bidder participation (Fazekas and Tóth 2016; Nemec et al. 2023). These are proxy indicators of corruption, since restricted competition and inflated pricing are generally recognised as manifestations of procurement corruption (Fazekas and Tóth 2016).
Transparency alone does not eliminate corruption risks. Undue influence by suppliers may still occur by changing the design of tender specifications (Bauhr et al. 2020: 7). Bauhr et al. therefore emphasise the importance of horizontal transparency, that is “transparency that provides information primarily to the parties involved in the bidding process rather than to outside observers” (Bauhr et al. 2020: 20), which equalises information among bidders and reduces insider advantage.
A major focus of procurement reforms in Central Asia is reducing single-source procurement and encouraging open competition. Uzbekistan provides one of the most ambitious examples. By 2030, the country aims to conduct 80% of its public procurement through competitive procedures (Frank.uz 2026). In 2022, over 41% of procurement contracts were awarded directly, without competitive procedures, already an important improvement compared to 2019 when was 70% (Subkhanov 2023: 2). Kazakhstan also shows very positive results in terms of competitive procurement. Direct awards dropped from 81% in 2017 to 23.5% in 2024, while suppliers’ participation has grown with the average number of bidders per lot rising from 3.16 in 2021 to 4.2 in 2024. Failed competitive tenders, once used as a workaround to justify direct awards, have also fallen from 52% of tender value in 2018 to just 3% by 2022–2024 (Tarnay and Bapakhova 2025).
Legal frameworks
A coherent and enforceable legal and regulatory framework is a precondition for reducing corruption risks in health procurement. Legal provisions that limit discretion, mandate transparency and clarify institutional responsibilities are consistently associated with improved procurement outcomes (Martini 2015).
Kazakhstan illustrates both the potential and limitations of legal reforms. Legislative changes, including reducing legal justification for single-source procurement, increasing penalties for public servants using direct procurement without due justification, and legalising civil society monitoring, contributed to reducing single-source procurement, expanded the publication of structured procurement data, and increased bidder participation and watchdog organisations’ monitoring (Tarnay and Bapakhova 2025). However, enforcement gaps in Kazakhstan remain. These include the absence of a debarment mechanism for corruption offences, allowing convicted individuals and companies to continue winning public contracts. Conflict of interest rules are also incomplete and do not cover all officials involved in procurement or extend to beneficial owners or subcontractors. Despite rules aimed at regulated single-source procurement, its use still exceeds the OECD recommended ceiling of 20% of procurement value (OECD 2024b: 113-122; OECD 2025a).
Oversight, enforcement and sanctions
Independent audits, whistleblower protection, sanctions and professional training remain essential across all procurement stages. In Uzbekistan, the procurement system implemented a system of monitoring and oversight that allowed the Anti-Corruption Agency to identify almost 500 instances of corruption just in the healthcare sector in 2025. The violations included bribery, abuse of official authority and nepotism across areas such as procurement, hiring and access to medical services. In response, authorities initiated criminal proceedings in some cases and applied disciplinary measures in others, including the dismissal of implicated officials and administrative sanctions within healthcare organisations (Yusupova 2026). Legal safeguards, secure reporting channels and capacity building for procurement officials can further reinforce such oversight and enforcement of these mitigation measures (Kohler and Dimancesco 2020; UNODC 2022).
Integrity in the pre-bidding phase
Transparency mechanisms such as publication of procurement plans and early disclosure of tender documentation can strengthen predictability and reduce discretion of procurement officials (OECD 2016; Bauhr et al 2019). Beneficial ownership transparency has emerged as an additional safeguard to prevent money laundering, corruption, and tax evasion, including in Central Asia where, for example, Kyrgyzstan and Kazakhstan authorities have established beneficial ownership registers (Council of Europe 2023a; Council of Europe 2023b). By requiring disclosure of ultimate beneficial owners, procurement authorities and auditors can identify related-party contracting and hidden conflicts of interest (Burr and Montalvo 2025). In one documented case in Ukraine, a civil society organisation cross-referenced official procurement records with beneficial ownership information obtained through government data requests and identified that a single individual had created multiple shell companies competing against each other in health procurement tenders, creating the appearance of competition while concealing a conflict of interest (AntAC 2013). Chile's recent procurement law reforms illustrate how beneficial ownership disclosure can be integrated into procurement eligibility requirements (Burr and Montalvo 2025). While empirical impact evidence remains limited, beneficial ownership transparency is widely recognised as strengthening oversight capacity (Brown 2025).
To mitigate the risks associated with information asymmetry and promote competition and price comparability, WHO governance assessments (2009: 87) recommend the use of International Non-proprietary Names (INN)93fdc5860546 rather than brand-specific requirements that can limit competition and increase prices (Vian et al. 2025: 11).
Recent reforms in Uzbekistan have the potential to mitigate risks at the pre-bidding stage through increased transparency and standardisation. From 2026, state procurement of medicines and medical devices will be centralised through a dedicated electronic module, with planned procurement volumes publicly disclosed through a national registry. In addition, participation will be restricted to manufacturers and distributors meeting recognised quality standards. Together, these measures aim to reduce information asymmetries between procuring entities and suppliers and to support more transparent and competitive tendering processes (Pharmaceutical Industry Development Agency, Ministry of Health, Republic of Uzbekistan, 2026).
Emergency procurement governance
Emerging good practices in emergency procurement recognise the need for both speed and transparency. Transparency must be central to all procurement decision-making even during crises; where emergency measures reduce the controls to prevent corruption, these should contain clear sunset clauses that enable legislatures to reassess and re-determine their continuance at regular intervals (Bruce 2020).
In practice this requires:
- clearly defined and time-bound derogations (exemption from or relaxations of standard procurement rules) with mandatory justification for their use;
- mandatory ex post publication of contracts and award decisions;
- disclosure requirements integrated into emergency e-procurement platforms; strengthened audit capacity during and after the emergency period; and
- active civil society engagement in monitoring, including through open-data tools and civic monitoring platforms of the kind deployed by Transparency International chapters in Argentina, Honduras and Ukraine (Transparency International 2023; Djumaev 2023).
The evidence also underscores that integrity infrastructure works best when built before a crisis hits: countries with pre-established procurement protocols, supplier registries, and civic monitoring capacity are significantly better positioned to manage corruption risks under emergency conditions (Jenkins et al. 2020; Griffore et al. 2023).
Digitalisation and e-procurement
Digital procurement platforms are frequently presented as anti-corruption tools. Review evidence suggests that electronic procurement (e-procurement) contributes to transparency, reduces discretionary human intervention and improves auditability across procurement phases (Mackey and Cuomo 2020; Saeed et al. 2022). However, Mackey and Cuomo (2020) note that adoption has been largely driven by cost-saving objectives, with anti-corruption goals remaining secondary. They recommend integrating defined anti-corruption indicators into health technology assessments of e-procurement systems, so that measuring cost savings can simultaneously serve as a proxy for detecting fraud or other irregularities (Mackey and Cuomo 2020: 10).
Ukraine’s ProZorro system provides one of the most cited examples. By combining digital tendering with open data publication and integration with the civic monitoring platform DoZorro, which directly accesses and displays procurement data for public oversight. DoZorro is run by Transparency International Ukraine and a network of civil society organisations, and it is accessible to citizens, businesses and authorities. ProZorro increased transparency, competition and enabled external scrutiny, contributing to saving almost US $6 billion in public funds between 2017 and 2021 (Yukins and Kelman 2022: 23). Early data indicates that over 2,000 health organisations in Ukraine saved an average of 15% on their procurement because they could access market data (Saeed et al. 2022: 6).
Similar platforms have been introduced in Kazakhstan, Kyrgyzstan, Tajikistan and Uzbekistan. In Tajikistan, open tendering reportedly accounted for a large share of procurement volume in 2021, and the government set ambitious targets for expanding digital coverage (Djumaev 2023).
While these results reflect implementation progress, they do not in themselves demonstrate corruption reduction. OECD documented continuing challenges related to data quality, oversight capacity and enforcement (OECD 2022). Moreover, the publication and digitalisation of data must be accompanied by sufficient capacity to review disclosures and identify potential red flags that may signal corruption. Simply making data publicly available does not, on its own, lead to an increase in corruption investigations; meaningful oversight requires dedicated bodies and organisations equipped to analyse the information effectively.
Legislative gaps may limit the impact of e-procurement reforms. For example, in Kyrgyzstan, the law on public procurement (2022) means that state-owned companies (one-third of all budget expenditure) are not required to hold tenders or publish public data on purchases (Tarnay 2022). Additionally, information on what government bodies buy and at what price is no longer published (Tarnay 2022). When data published by state‑owned enterprises is incomplete, the benefits of e‑procurement are significantly weakened.
Emerging technologies
Emerging technologies such as artificial intelligence (AI) and blockchain are increasingly applied as integrity tools (Resimić 2025). AI can detect fraudulent patterns in medical insurance, identify counterfeit pharmaceuticals through image recognition and network pattern analysis across supply networks, and flag irregularities in procurement processes. Its effectiveness depends on how and by whom it is deployed: governments may use it for oversight, risking abuse of power, while civil society may use it for accountability, facing data and misinformation challenges. It may also be manipulated to facilitate illicit activities, for example by feeding skewed data, or to reinforce unequal power dynamics, for example if trained on biases from historical data (Rey-Puech et al. 2025: 1344).
Blockchain is a distributed ledger technology that creates records that cannot be easily altered. It offers potential for tracking pharmaceutical supply chains and detecting falsified medicines (Mackey and Cuomo 2020; World Economic Forum 2020). Blockchain pilots in other sectors — such as Colombia's school feeding programme — have demonstrated that distributed ledgers can reduce opacity and create audit trails that can reduce reliance on centralised authorities, while smart contracts can automate and enforce process steps without human discretion (World Economic Forum 2020: 5-6). However, blockchain cannot address corruption or falsification that occurs outside electronic systems, such as collusion among supply chain actors (World Economic Forum 2020: 28-35).The potential for similar applications in pharmaceutical supply chain monitoring is evident from the many pilots and proof-of-concept projects proposed by start-ups, technology companies, and multilateral organisations, though actual implementation at scale remains elusive, especially in low and middle-income countries, alongside unresolved challenges in privacy and integration with existing systems. Blockchain technology is also explored as a tool in e-procurement to potentially enhance transparency and reduce discretion in purchasing decision (Belokurova et al. 2022).
In Brazil, a coalition of government agencies and civil society organisations is using open data and AI to improve transparency in pharmaceutical procurement (Lopez et al. 2026). Launched in 2025, the platform Medicamentos Transparentes aggregates medicine purchases from over 5,000 municipalities and 27 states, previously scattered across 263 separate systems, into a single, publicly accessible portal. It uses a large language model to clean and standardise procurement records, enabling price comparisons across regions and over time. This standardisation allows to compare unit prices for identical or equivalent medicines, identify price variations across regions, and flag potential anomalies for further investigation. Public officials use these comparisons to establish reference prices when designing or evaluating tenders, while civil society and journalists can use the platform to monitor spending, detect unusually high prices and investigate procurement anomalies. Early results are promising. The platform successfully matched 80% of medicine procurement items to standardised codes using AI, compared to just 5% previously, significantly increasing the share of procurement data that can be meaningfully compared across jurisdictions (Lopez et al. 2026).
Citizen-led digital platforms are also emerging to support anti-corruption efforts in health procurement by encouraging participation (Open Contracting Partnership 2025). In Kyrgyzstan, the platform Tsa.Kallow users to monitor public procurement procedures by automatically retrieving daily tender data from the official procurement website. Users can analyse bids, check participation requirements, file complaints, track contract awards and monitor budget spending, while moderators flag potential violations. In Kazakhstan, the AI-based platform Datanomix.pro has been deployed to detect fraud and misconduct in procurement data, offering a tool for identifying red flags that is accessible to civil society (Open Contracting Partnership 2025).
The deployment of an AI-powered tool that compares tender data with average market prices to flag risks is being planned as part of the new procurement reforms in Uzbekistan (Sultanova 2026).
Open contracting and data transparency
Open contracting initiatives such as the Open Contracting Data Standard (OCDS) promote structured, machine-readable publication of procurement data throughout the contracting process, enabling systematic identification of risk indicators such as limited competition or frequent contract amendments.
In Kazakhstan, the integration of OCDS in the central procurement platform contributed to reducing direct awards to 23.5% of procurement value and increased the average number of bidders from 3.16 to 4.2 (Tarnay and Bapakhova 2025). The number of legal exceptions permitting direct awards was reduced from 67 to 43. Penalties for violations were strengthened, and the failed-tender loophole that previously allowed automatic reversion to single-source methods was closed. Nevertheless, enforcement of penalties is inconsistent, criminal prosecution data is limited, and some non-competitive categories were quietly reintroduced in 2025 in the new Law on Public Procurement (Tarnay and Bapakhova 2025).
Transparency International Global Health's Open Contracting for Health (OC4H) programme in Zambia demonstrates that expanded procurement disclosure at local government level, combined with stakeholder training across government and the private sector, can help build civil society monitoring networks. The programme introduced open contracting tools and capacity-building that enabled CSOs to access and interpret procurement data, supporting basic monitoring of selected health procurement cases and engagement with local authorities on procurement decisions. Cross-cutting activities also included advocacy and dissemination of procurement transparency messages through media, community engagement, and stakeholder platforms, and collaboration with journalists and media actors to support investigative use of procurement data. (Transparency International Global Health 2021; Transparency International Global Health n.d.).
Participatory oversight: Integrity Pacts and civic monitoring
Participatory mechanisms complement formal regulation by increasing transparency and reputational accountability. Integrity Pacts (IPs), developed by Transparency International, consist of a public agreement between public contracting authorities and suppliers to apply specific transparency, accountability and integrity measures in one or all of public contracts (Transparency International n.d.). As part of this agreement, an independent monitoring mechanism is led by civil society to oversee compliance with laws and regulations and report irregularities to oversight institutions (Transparency International n.d.).
IPs have been implemented in a range of countries in Europe, as well as in India, Pakistan and Mexico, in public sector procurement contexts12 (Transparency International n.d.). In Uzbekistan, an integrity pact constitutes a core requirement of an ongoing development project on climate resilience and water, sanitation, and hygiene (WASH) infrastructure in schools (The Times of Central Asia 2025b). However, due to limited civic space and restricted independent oversight in the Central Asia region, participatory tools such as Integrity Pacts may face greater constraints.
In Honduras, an IP, signed by the Ministry of Health and major pharmaceutical companies, was implemented for medicine procurement (2017–2021) following a corruption scandal that revealed large quantities of medicines, worth millions of dollars, had been taken from the central medicines warehouse and were likely sold on the black market. External actors that provided services to the Ministry, such as the College of Chemists and Pharmacists of Honduras and Banco de Occidente, signed an ethics statement. By introducing independent civil society monitoring and mandatory anti-bribery commitments, the initiative doubled the number of pharmaceutical suppliers and increased price transparency, contributing to fairer costs and better value for money in the healthcare system (Basel Institute on Governance n.d.). Similarly, evaluations of IP initiatives in Europe suggest improvements in procedural compliance and strengthened stakeholder trust (Transparency International 2015; European Commission 2020), although quantitative evidence of direct reductions in corruption is not available.
Civic monitoring platforms, such as Ukraine's DoZorro, also enable civil society actors to exercise additional oversight over public procurement processes. Research indicates that combining open data with participatory monitoring increases the detection of red flags and may contribute to corrective action (Open Contracting Partnership 2019). In Kazakhstan, civic monitoring of COVID-19 emergency procurement identified dubious medical equipment contracts and price-fixing in food stabilisation funds, prompting multiple investigations into suspect public spending (Eurasia Foundation 2021). Similar dynamics have also been documented in the Western Balkans, where investigative journalism has played a comparable oversight role. In North Macedonia, for example, the Investigative Reporting Lab (IRL), a nonprofit newsroom focusing on corruption and governance, investigated a 2021 fatal fire at a temporary COVID-19 health facility in Tetovo. IRL exposed corruption in the public procurement of modular health infrastructure, revealing weaknesses in contracting controls and accountability gaps in public spending (GIJN 2023).
Adjacent to civic monitoring, media scrutiny can constitute an important corruption detection mechanism. In Kazakhstan, another procurement scandal during the COVID-19 pandemic was uncovered through investigative reporting (Satke 2021). The Organized Crime and Corruption Reporting Project (OCCRP) platform investigated the country’s accountability mechanism and found that there was no detailed information on where the US$645 million of emergency funds went, as the Kyrgyz government had failed to sustain the transparency policy (Satke 2021). A later investigation by Kyrgyz journalists from the group Politklinia also found that, shortly before the COVID-19 pandemic, the prices for personal protective equipment and medical masks had been over inflated (Satke 2021).
Multi-stakeholder transparency initiatives
Past initiatives such as WHO's Good Governance for Medicine (GGM) and the Medicines Transparency Alliance (MeTA) brought together governments, civil society and the private sector to improve procurement transparency.
MeTA operated between 2008 and 2025 in seven countries, including Kyrgyzstan, to increase access to medicines through enhanced transparency and accountability in policy discussions. Documented outcomes include increased disclosure of pharmaceutical information and reforms to procurement pricing and standard bidding documentation. In Kyrgyzstan, MeTA contributed to shaping the State Medicines Policy, supporting inter-sectoral coordination and improving monitoring systems (Vian et al. 2017: 6–7).
According to Vian et al. (2017), MeTA was largely successful in achieving its stated objectives, including reducing corruption (Vian et al. 2017: 8). However, the long-term impact on government performance depends on whether institutionalised transparency measures are sustained over time. As Wong et al. (2024) also note, many participating countries adopted the mandatory UNCAC provisions — such as criminalising bribery — but were slower to adopt non-mandatory provisions such as whistleblower protection or criminalisation of private sector bribery (Vian et al. 2017: 10).
Summary: risks and mitigation mechanisms across the procurement cycle
While the approaches discussed above are organised thematically, they address vulnerabilities that arise at different stages of the procurement cycle. Table 2 summarises how key corruption risks and mitigation mechanisms relate to the main stages of public health procurement.
Table 2: Procurement Stages, Risks and Mechanisms
|
Procurement Stage |
Common corruption risks |
Anti-corruption/Mitigation mechanism |
|
Governance environment |
|
|
|
Pre-bidding (needs assessment, planning, specification, tender design) |
|
|
|
Bidding and contract award |
|
|
|
Post-bidding (contract implementation and oversight) |
|
|
|
Emergency procurement (cross-cutting across all stages) |
Compressed accountability timelines |
Reinforced conflict-of-interest controls |
Conclusion
The evidence reviewed points to several common success factors: sustained political will, meaningful engagement of civil society and the private sector through trainings and multi stakeholder initiatives, transparency through open data and digital tools, and independent public oversight with genuine enforcement capacity. Where these elements align, reforms are more likely to move beyond formal adoption to achieve meaningful compliance and, ultimately, real improvements in procurement integrity.
Yet persistent challenges remain. Weak governance structures, limited civic space, insufficient oversight capacity, incomplete digitalization and data access gaps constrain both prevention and detection. Procedural red flags are valuable diagnostic tools, but they cannot on their own capture deeper structural drivers, elite capture, power asymmetries, and institutional weaknesses, that shape how corruption manifests in practice and may limit the effectiveness of technical fixes if left unaddressed.
In Central Asia, three aspects of reform seem promising: digitisation and related reforms for expanded e-procurement; incremental institutional reform; and greater civic and private sector engagement. Kazakhstan and Uzbekistan have pursued comparatively more ambitious reform trajectories than the other countries in the region, significantly reducing single-source procurement and expanding e-procurement coverage. Yet enforcement gaps in debarment procedures and conflict-of-interest rules limit the accountability impact of these advances. Progress is further constrained by weaknesses in data quality, reflecting incomplete implementation of digitalisation due to capacity and funding limitations, and the underuse of available data to detect irregularities.
In Kyrgyzstan, the dominant role of a single state-owned pharmaceutical distributor creates structural centralisation risks that current oversight arrangements do not adequately address, while reforms in Tajikistan and Turkmenistan remain more limited in scope. Across the region, constrained civic space means that domestic participatory oversight mechanisms carry less weight than in more open political environments, making international monitoring frameworks such as OECD peer review, donor conditionality, and open contracting partnerships, particularly important accountability levers.
- By strengthening efficiency, fairness and market integrity, it also contributes to broader policy goals, including SDG 10 on reduced inequalities, SDG 8 on decent work and economic growth, and SDG 12 on responsible consumption and production (OECD 2024; Bruckner 2019).
- This also includes the WHO Prequalification Programme (PQP), which certifies the quality, safety and efficacy of medicines, vaccines and diagnostics eligible for procurement (WHO no date); and the Model List of Essential Medicines (EML), which defines the reference set of medicines that health systems should prioritise (WHO 2023a).
- While this Helpdesk Answer examines Central Asia as a region, it is important to note that this region is not a uniform governance space. There are different procurement systems, oversight capacity, civic space and media freedom in each of the countries which each has a different impact on corruption risks.
- The Central Asian region is widely considered to denote the five republics of Kazakhstan, Kyrgyzstan, Tajikistan, Turkmenistan, and Uzbekistan.
- UNCAC refers to public procurement more generally.
- The IAP is a regional programme launched by the OECD in 2003 to support anti-corruption reforms through peer reviews, recommendations, and monitoring of reforms (OECD, 2003). The OECD has been invited to carry out assessments of Kazakhstan, Kyrgyzstan, Tajikistan and Uzbekistan, but not Turkmenistan.
- This figure is an estimate and does not necessarily accurately reflect the yearly cost of corruption, fraud and waste to the sector.
- Fraud is the “offence of intentionally deceiving someone in order to gain an unfair or illegal advantage (financial, political or otherwise)”. Countries treat fraud as either a crime or a violation of civil law (Transparency International n.d.)
- In the World Press Freedom Index, Kazakhstan is listed in 141th place, Kyrgyzstan 144th, Uzbekistan 148th, Tajikistan 153th and Turkmenistan 174th out of 180 countries.
- For more information on the strengths and weaknesses of decentralised procurement models in the health sector, as well as an overview of such systems in practice, see Millington, K.A. and Bhardwaj, M. 2017. Evidence and experience of procurement in health sector decentralisation.
- Fraud is the “offence of intentionally deceiving someone in order to gain an unfair or illegal advantage (financial, political or otherwise)”. Countries treat fraud as either a crime or a violation of civil law (Transparency International n.d.) online here.